VICKI SIMS, PT CHT
DAVID MESNICK, PT
ALAN LIPPITT, MD
MICHAEL AMARAL, MD, FACS
550 Peachtree Street, Suite 1760
Atlanta, Georgia USA 30308
(404) 817-0734
dmesnick@afptc.com
INTRODUCTION
Disruption of the sacroiliac joint is recognized as a potential source of spine and pelvic pain. Unfortunately, there is no standard objective study to demonstrate this.
The physiopathology is a tearing or stretching of the posterior sacroiliac ligament complex with subsequent
hypermobility. In the more severe cases, destabilization can lead to recurrent subluxation, disruption of gait, and a breakdown in the balance of ligaments and muscles. This leads to significant impairment.
Imaging studies such as MRI, bone scanning, plain x-ray, or CAT scans do· not image abnormalities in the ligamentous support system of the Sacroiliac joint.
Color Doppler Imaging (CDI) is a reliable means of measuring joint stiffness and, therefore, a method of determining hypermobility. Asymmetry in joint stiffness of the Sacroiliac joint is the most important factor in determining pelvic pain (Damen, 2002).
The authors have determined that sacroiliac stabilization is important in relieving the physiopathology of sacroiliac instability. Various methods have been developed to stabilize the joint
including belting, muscle balancing, taping, prolotherapy, and surgical intervention. These modalities are well covered elsewhere.
The purpose of this study is to evaluate the stiffness level of the sacroiliac joints before and after surgical stabilization, either by percutaneous screw fixation or by fixation and bony fusion. Further testing will attempt to correlate joint stiffness and pain.
MATERIALS AND METHODS
Color Doppler imaging (CDI) measurements were performed pre and post operatively on the SIJ of 10 female, and 3 male subjects. The diagnosis of SIJ laxity was based on manual testing. Confirmation of the joint as a pain generator was determined with a fluoroscopically controlled intra-articular block.
The subjects were placed in the prone position with muscles relaxed. Vibrations (frequency 200 Hz, amplitude not exceeding 0.05 mm and excitation power 1.5 w) were applied unilaterally to the anterior superior iliac spine (ASIS). A Homedics PA-2004 vibrator generated the vibrations. The vibrations traveled from the anterior aspect of the ilium to the SIJ. The intensity of the vibrations was measured across the ipsilateral SIJ with CDI. On the dorsal side, a 7.5 MHz transducer was positioned perpendicular to the body axis and the intensity of vibrations measured successively on iliac and sacral sides of the SIJ.
When the threshold button was selected the” tester was able to adjust the Doppler threshold before vibration was depicted as flow. When the threshold was reached, the vibrations were displayed as red and blue on the CDI monitor. Below this level, conventional gray scale B-Mode images were displayed. A comparative measurement was performed between the ilium and sacrum. First, a threshold level was measured from the sacrum when the color pixel disappeared and changed to gray scale. Next, a second threshold level was measured for the ilium. The threshold level was directly related to the vibration of the bone. A large difference between the threshold levels of the sacrum and ilium indicated a large loss of energy through the SI joint and, therefore, a low stiffness value. A small difference between the threshold levels of the sacrum and ilium indicated a small loss of energy through the SI joint; and therefore a high stiffness value. Stiffness was quantified by using Buyruk’s scale of Threshold Units (TU). High stiffness was <3 TU, intermediate stiffness was 3-7 TU, and low stiffness was >7 TU. The test was repeated three times on each sacroiliac to determine intra-tester reliability. The same tested was used for all 13 subjects (26 total runs with one on the left SIJ and one the right SIJ for each subject). The measurements were performed the day before surgical intervention and then again within 4 weeks after the surgery. Only patients that failed conservative modes of treatment were considered for surgery.
Surgical technique
The SIJ was placed in anatomical alignment using manual techniques and muscle energy. The surgery was done under general anesthesia and with the patient in the prone position. Using fluoroscopic control, titanium orthopedic screws were tightened through the ilium into the ala of the sacrum. Depending on the patient’s symptomatology and degree of preoperative ligament laxity, a posterior sacroiliac bone fusion was also performed. Subjects received either unilateral or bilateral surgical stabilization depending on their diagnosis.
RESULTS
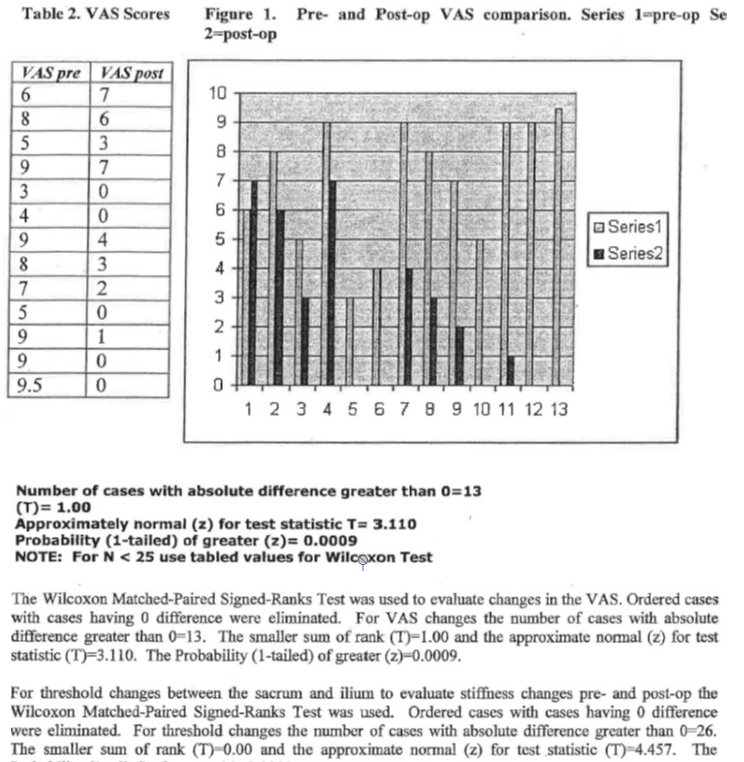
Different levels of stiffness were measured in Threshold Units (TU) and observed before and after the specified surgical intervention. Table 1 shows the difference in threshold levels on the ilium and sacrum of each side of the SI joint pre- and post-surgical stabilization. Table 2 compares scores on the Visual Analog Scale (VAS) pre- and post-op a 6 weeks. Figure 1 shows changes from series 1 (pre-op) to series 2 (6-weekspost-op).
Table 1.
Threshold difference between the ilium and sacrum. Measurements are given in Threshold Units (TU).
The average of 3 measurements per side was used pre and post-op.
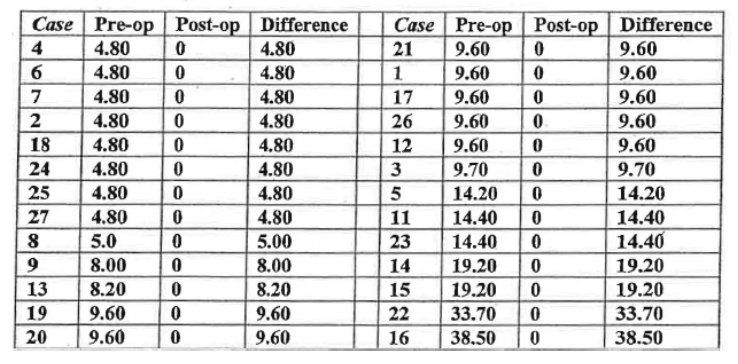
<3 High Stiffness
3-7 Intermediate Stiffness
>7 Low Stiffuess
• Number of cases with absolute difference greater than 0=26
•(T)= 0.00
•Approximately normal (z) for test statistic T= 4.457
•Probability (1-tailed) of greater (z) = 0.0000
•NOTE: For N < 25 use tabled values for Wilcoxon Test
DISCUSSION
SIJ laxity can be significantly changed by sacroiliac stabilization surgery
This study revealed a significant change in SI joint stiffness between measurements taken pre- and postoperatively. In every case the surgical intervention resulted in higher joint stiffness, which effectively eliminated movement (see Table 1). These changes were the result of surgical intervention. To date, follow-up studies have not assessed the long-term stiffness value changes. It is presumed that unless a subject sustained a new injury then his stiffness value should remain the same over time.
SIJ laxity is directly related to low back and pelvic pain and decreases with surgical stabilization.
Table 2 and Figure 1 represent a significant change on the VAS following surgical stabilization. LBP and pelvic pain that was present pre-operatively decreased in most cases following surgical stabilization. Surgical stabilization was shown to increase the stiffness of the SIJ in every case and therefore can be presumed to be the reason for a decrease in pain as recorded on the VAS post-surgically.
CONCLUSION
Stiffness measurements using Color Doppler Imaging is successful on human SI joints with good success. This method can provide objective, repeatable measures with statistical significance. CDI testing can be used in patients previously diagnosed with SIJ instability to confirm asymmetrical ligamentous laxity. This test is an objective measure that can be helpful in determining the need for sacroiliac surgical intervention. This test is effective in determining changes in SI joint stiffness following surgical stabilization. This study confirms an increase in SI stiffness across the affected joint in subjects who underwent surgical stabilization. VAS changes correlate increased joint stiffness with decreased pain.
REFERENCES:
Darilen L., Buynik, H.M., Guler-Uysal F, Lotgering F K, Snijder C J, Starn H J 2002b Prognostic value
of asymmetric laxity of the sacroiliac joints in pregnancy-related pelvic pain. Spine 27 (24):2820
Buyruk, H.M., Stam H.J. Snijder, C.J., Vlemming, A., Lameris, J.S., Holland, Stam H J 1995b
The measurements of sacroiliac joint stiffness with colour Doppler imaging: a study on healthy subjects.
European Journal of Radiology 21:117
Buyruk, H.M., Stam H.J., Snijder, C.J., Vlemming, A., Lameris, J.S. Stijnen W P 1999
Measurement of sacroiliac joint stiffuess in peripartum pelvic pain patients With Doppler imaging of
vibrations (DIV). European Journal Obstetrics Gynecological Reproductive Biology 83 (2): 159
Buyruk, H.M., Stam H:J., Snijder, C.J., Vlemming, A., Lameris, J.S., Holland, W.P .J.: The use of
colour Doppler Imaging for assessment of sacroiliac joint stiffness: a study on embalmed human pelvises.
European Journal of Radiology 21 (1995) 112-116.
Lee, D: An Integrated model of “joinf’ function and its clinical application. Fourth Interdisciplinary
World Congress on Low Back & Pelvic Pain. pp 137-152,2001.
Leonie, D., Buyruk, H.M., Guler-Uysal, F., Lotgering; F.K., Snijders, C.J., Stam, H.J.: Pelvic pain
during pregnancy is associated with asymmetric laxity of the sacroiliac joints. Asta Obstetricia et
Gynecologica Scandinavica. pp 1010-1024,2001.
Leopie, D. Stunen, T., Roebroeck, M.E., Snijders, C.J., Stam, H.J.: Reliability of Sacroiliac Joint
Laxity Measurements with Doppler Imaging of Vibrations. Ultrasound in Med. & Biology, Vol. 28, No.4,
pp 407-414m 2002.
Lippitt, A.B.: Recurrent Subluxation of the sacroiliac joint: diagnosis and treatment. Bulletin
Hospital for Joint Diseases. Vol. 54, Number 2. 94-102, 1995.